
SZARVAS LAB
Molecular factors in Uro-Oncology
The therapeutic landscape of urological tumors is rapidly evolving, making clinical decision-making increasingly complex. Currently, therapy choices are predominantly determined by clinicopathological parameters. However, patients with similar clinicopathological characteristics often exhibit significant individual differences in therapy sensitivity. Molecular factors have been demonstrated to influence the biological and clinical behavior of certain tumors. Therefore, a deeper understanding of the underlying mechanisms will facilitate the improvement of therapeutic sequences, ultimately leading to better patient outcomes
Prof. (apl) Dr.
Tibor Szarvas
Head of Uro-Oncology Group
Urothelial carcinoma
Molecular subtypes
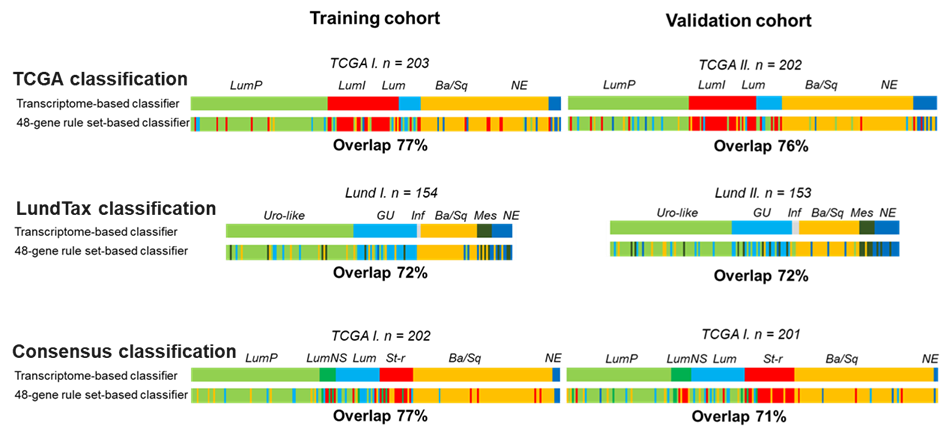
Histologically similar muscle-invasive urothelial tumors exhibit remarkable heterogeneity in their gene expression profiles. This diversity has led to the classification of urothelial carcinomas into molecular subtypes. Currently, six molecular subtype classification systems are employed, relying on whole transcriptome sequencing analysis. However, this method is expensive, technically challenging, and requires high amounts of input RNA, making it impractical for routine use. Therefore, our research group has developed a novel gene panel-based approach which is compatible with real-time qPCR and NanoString analysis platforms.
Olah et al. Int J Cancer 2021
Platinum-based chemotherapy
Olah et al. Cancer Med 2022
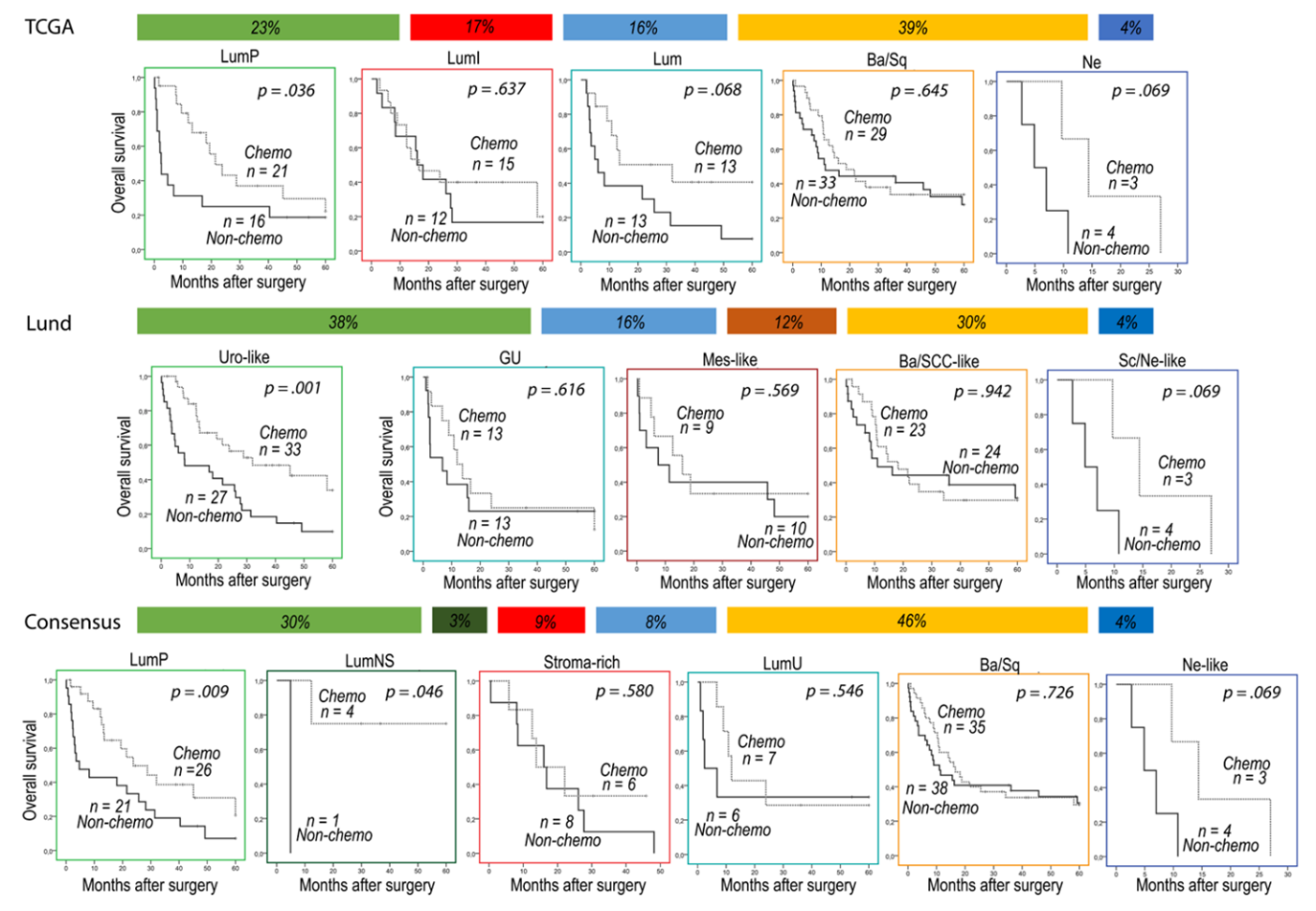
Perioperative platinum-based chemotherapy is still the standard treatment for muscle-invasive bladder cancer. However, urothelial carcinoma is a platinum sensitive disease, only 50% of patients benefit from the treatment, while its toxicity is high. In addition, alternative treatment options both preoperative and postoperative settings are available. Therefore, prediction of platinum therapy is of paramount clinical importance. Our research group applying a systematic proteomics approach identified potential tissue and serum markers for platinum-resistance and assessed the platinum predictive value of molecular subtypes. We found that luminal rather than basal subtype tumors are more sensitive to adjuvant platinum treatment.
Immune checkpoint inhibitor (ICI) therapy
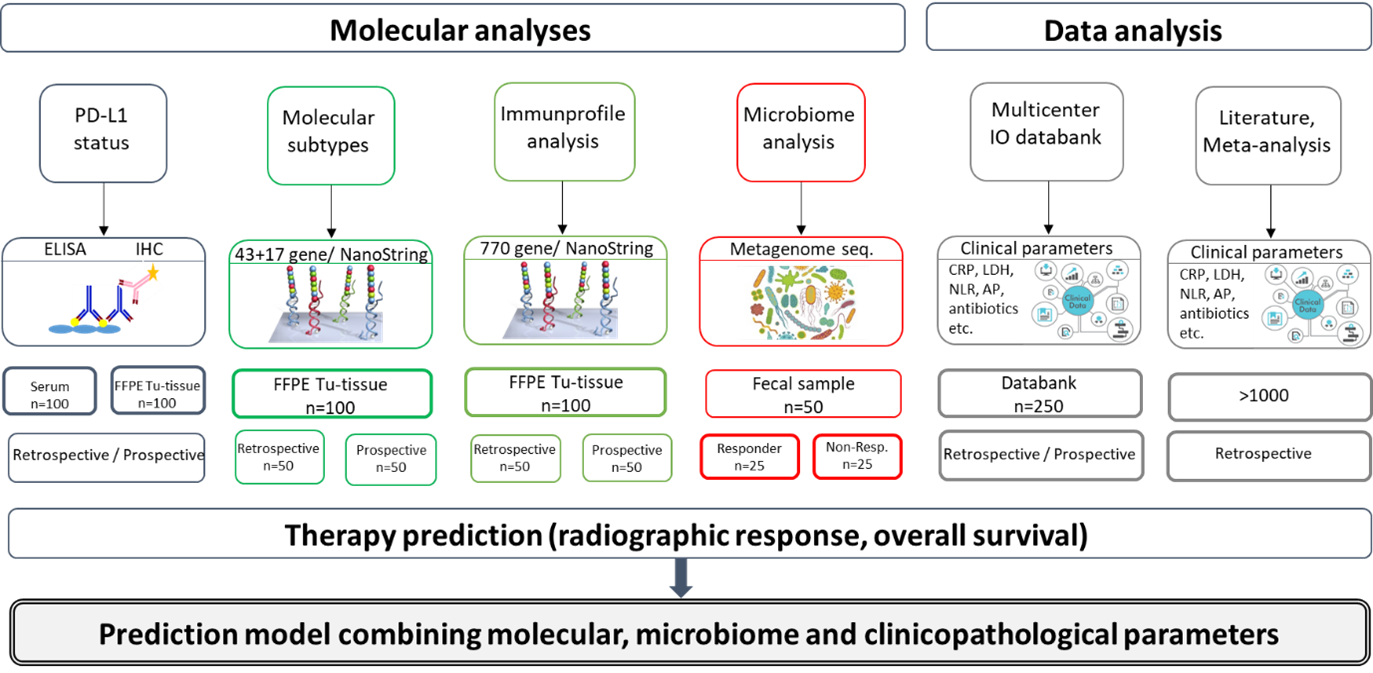
Currently, ICI therapy can be administered to patients with platinum-sensitive, resistant, or ineligible advanced urothelial carcinoma. While this therapy may offer long-term survival for responsive patients, only a relatively small subgroup (15-30%) derives benefit from it. Currently, PD-L1 immunohistochemistry is the only predictive marker utilized, however its negative predictive value is insufficient and therefore better predictive markers are needed. To address this need, we conducted a multicenter data and sample collection study of urothelial carcinoma patients who underwent ICI therapy. Additionally, we conducted meta-analyses of potentially predictive blood-based markers. Finally, we performed molecular gene expression analysis for molecular and immunologic subtype classification, as well as molecular microbiome analyses, in order to identify molecular and microbiota correlates of ICI sensitivity.
Krafft et al. Cancers 2021
Széles et al. Cancer Immunol Immunother. 2022
Szarvas et al. European Urology Open Science, 2023
Váradi et al. European Urology, 2023
Váradi et al. SciRep, 2023
Enfortumab vedotin
The use of antibody-drug conjugates targeting either with nectin-4 (enfortumab vedotin) or Trop2 (sacituzumab govitecan) represent a new class of drugs in the treatment of urothelial carcinoma. As both of these therapies are not yet widely used, real-world data for the identification of clinically defined subgroups with differential treatment sensitivity is necessary. Therefore, we conducted a systematic review and meta-analysis of the published literature to answer the above question. In addition, ongoing research focuses on the expression of these therapy targets in rare bladder cancer entities.
Prostate cancer
Prostate cancer is largely heterogeneous, with clinical presentations ranging from indolent tumors to locally advanced but hormone-sensitive, and progressing to aggressive castration-resistant and metastatic stages.
Prognostic stratification of localized prostate cancer
In clinically localized prostate cancer, there is still an unmet clinical need to differentiate between early-stage but high-risk and indolent cases. Since early detection of prostate cancer in asymptomatic stages often leads to overtreatment, population-based screenings are currently not recommended by professional guidelines. Therefore, prognostic markers are necessary to better stratify patients and support prostate cancer screening efforts. In a recent study, we conducted a systematic in silico evaluation of published prostate cancer datasets to identify prognostic tissue factors. Ultimately, we identified and validated three tissue markers that were capable of enhancing the currently employed clinical risk models.
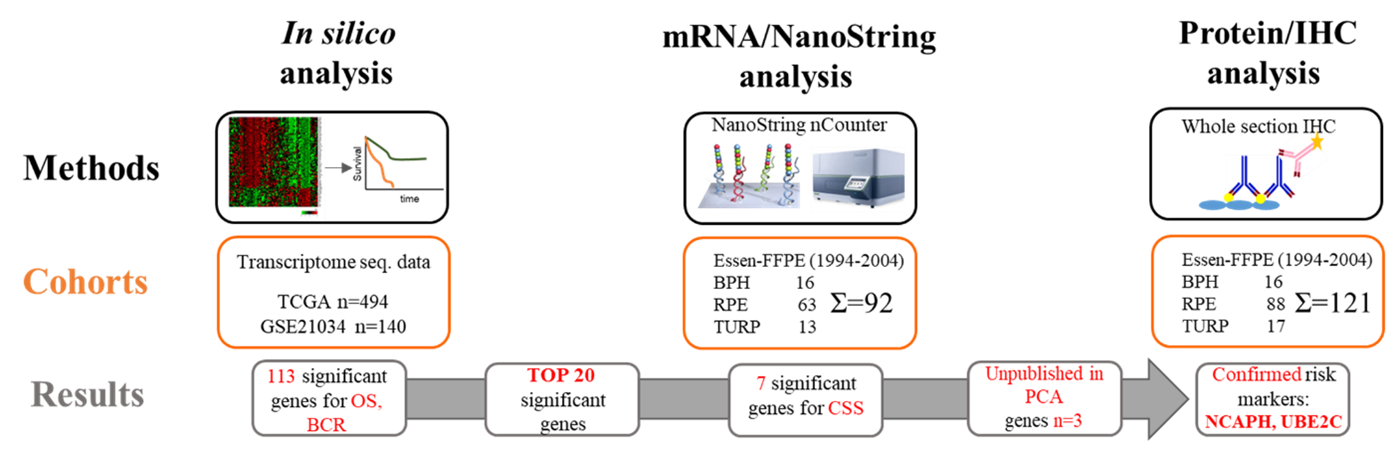
Olah et al. European Urology Open Science 2023
Keresztes et al. J Cell Mol Med 2022,
Csizmarik et al. Int J Cancer 2022,
Csizmarik et al. Prostate Cancer Prostatic Dis 2023
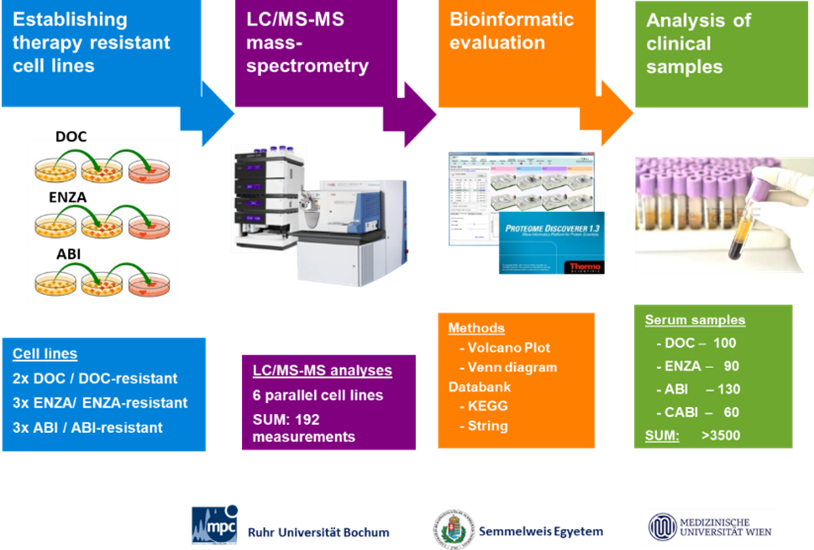
Androgen Receptor targeting agents (ARTA)
ARTAs are widely used in advanced prostate cancer. However, for metastatic castration-resistant prostate cancer, there is an increasing number of systemic therapies with various mechanisms of action available. Therefore, predicting therapeutic sensitivities on an individual level is becoming increasingly important. To address this, we conducted a comparative proteome analysis between abiraterone, enzalutamide, and docetaxel-sensitive versus resistant prostate cancer cell lines. We then identified differentially expressed proteins in serum samples from patients with mCRPC who underwent these therapies.
Neuroendocrine-differentiated prostate cancer cells are found in virtually all prostatic adenocarcinomas. Since these cells are less responsive to antiandrogen therapies, they face selective pressure under androgen deprivation therapy. Consequently, castration-resistant prostate cancers become enriched in neuroendocrine tumor cells through a process called neuroendocrine transdifferentiation. Diagnosing this phenomenon is challenging, but certain neuroendocrine serum markers may aid in identifying cases with enhanced neuroendocrine transdifferentiation. In a comprehensive analysis, we determined the serum levels of two neuroendocrine serum markers (chromogranin A and neuron-specific enolase) and found that patients with high serum levels before systemic therapy benefited more from docetaxel chemotherapy than from ARTA treatment.
Szarvas et al. BJUI 2021
PARP inhibitor treatment
Prostate cancer patients who present with BRCA1/2 or other homologous recombination repair (HRR) gene mutations represent a clinically distinct molecular subtype of prostate cancers. BRCA-positive prostate cancers are typically diagnosed at younger ages, progress more rapidly under androgen deprivation therapy, and have a poorer prognosis. Conversely, HRR-deficient patients tend to derive more benefit from platinum-based chemotherapies as well as from targeted PARP inhibitor (PARPi) therapies. To gain a better understanding of the therapeutic sensitivity of this molecular subtype, we conducted two systematic reviews and meta-analyses. Our findings revealed that BRCA-positive patients demonstrate a higher PSA50 response when treated with enzalutamide compared to abiraterone treatment. Additionally, platinum-based therapies exhibited comparable efficacy to PARPi. Since real-world therapeutic experience for this patient group is still limited, we conducted a multicenter data collection study.
Fazekas et al. Prostate Cancer Prostatic Dis 2022
Fazekas et al. Eur Urol Oncol 2023
Urachal carcinoma
Urachal carcinoma is a rare tumor that is mostly diagnosed in advanced stages when systemic treatment is required. However, due to the lack of prospective clinical trials, there are no guidelines or treatment recommendations available, making therapeutic decisions extremely challenging.
Epidemiology
Only sparse data are available on the incidence of urachal carcinoma. Therefore, we conducted cancer registry-based analyses using data from the Robert Koch Institute in Germany and the National Cancer Registry in Hungary. Additionally, we performed a systematic review and meta-analysis on registry-based studies for urachal carcinoma, determining a median incidence of 0.04 per 100,000 inhabitants per year, with substantial differences between various countries. Further research is needed to identify the reasons for these differences, which may help identify the yet unknown risk factors of this enigmatic disease.
Hager et al. Urol Int 2020
Olah et al. Urol Oncol 2024
Clinicopathological parameters and therapy sensitivity
In two comprehensive systematic literature reviews, we extracted data on the clinicopathological patterns, treatment modalities, and immunohistochemical characteristics of urachal carcinoma. Our findings revealed that the combination of 5-Fluorouracil (5-FU) and platinum therapy offers the highest efficacy in terms of radiographic progression. This was followed by 5-FU-based modalities without platinum, while platinum therapies without 5-FU exhibited the lowest efficacy.
Szarvas et al. Urol Oncol 2016
Reis et al. Biomarkers 2018
Targeted treatment options
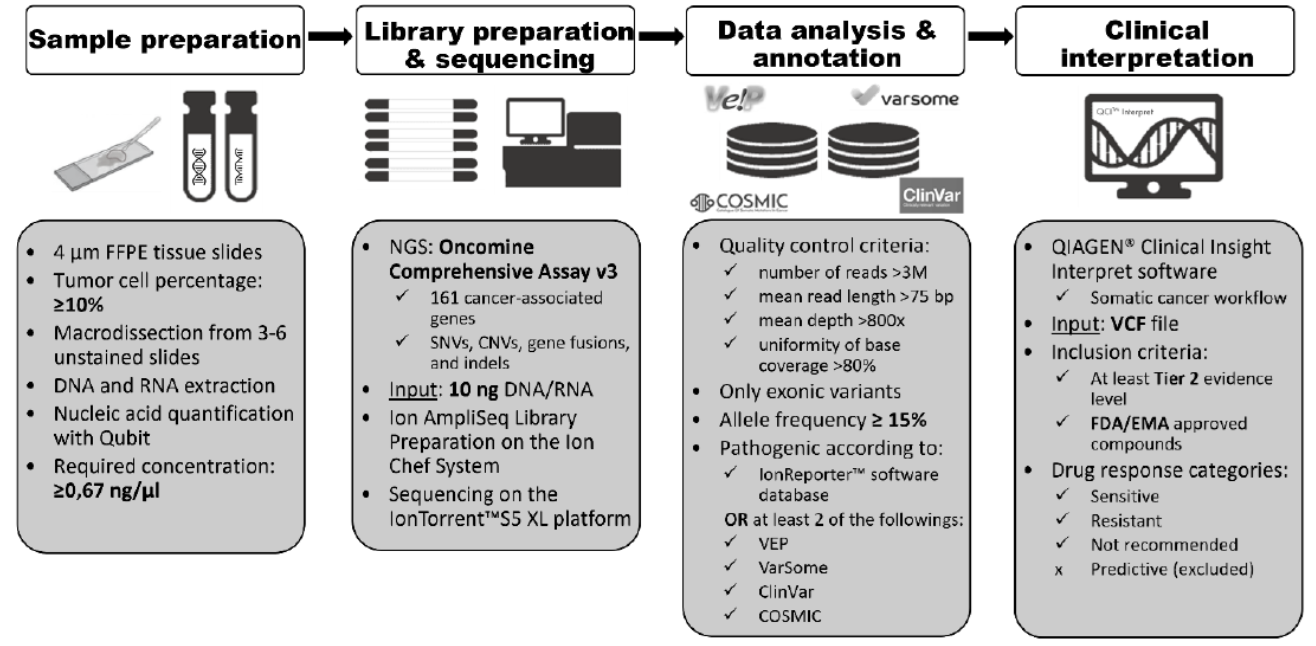
Váradi et al. Cancer Med 2023
For rare cancers lacking prospective clinical trials and clear therapeutic recommendations, an individual mutational pattern-based precision medicine approach represents a reasonable treatment strategy. To implement this, a better understanding of the mutational pattern of urachal cancer is necessary. In recent years, we conducted an international sample and data collection across several European countries. Utilizing commercially available oncological DNA sequencing panels and a clinical annotation tool, we assessed the applicability of targeted treatment approach in urachal cancer. Our findings revealed that we were able to identify at least one targetable alteration in over 90% of urachal cancer patients.